Parenteral medication administration is an effective method of delivering medication to patients, and it can be safely accomplished by utilizing the appropriate guidelines and policies in place to keep patients safe from harm. IV medications have a higher risk of harm than non-parenteral medication. The ever-increasing complexity of the health care environment increases the risk of a medication error with parenteral medications. The key takeaways below provide advice for preventing errors with parenteral medications.
Key Takeaways
- Parenteral medications have a relatively quick onset of therapeutic effects. Be aware of the onset, peak, and duration of all parenteral medications.
- Know which medications are considered high-alert medications, and perform independent double checks to minimize errors.
- Always consider the therapeutic effects and adverse effects when administering parenteral medications.
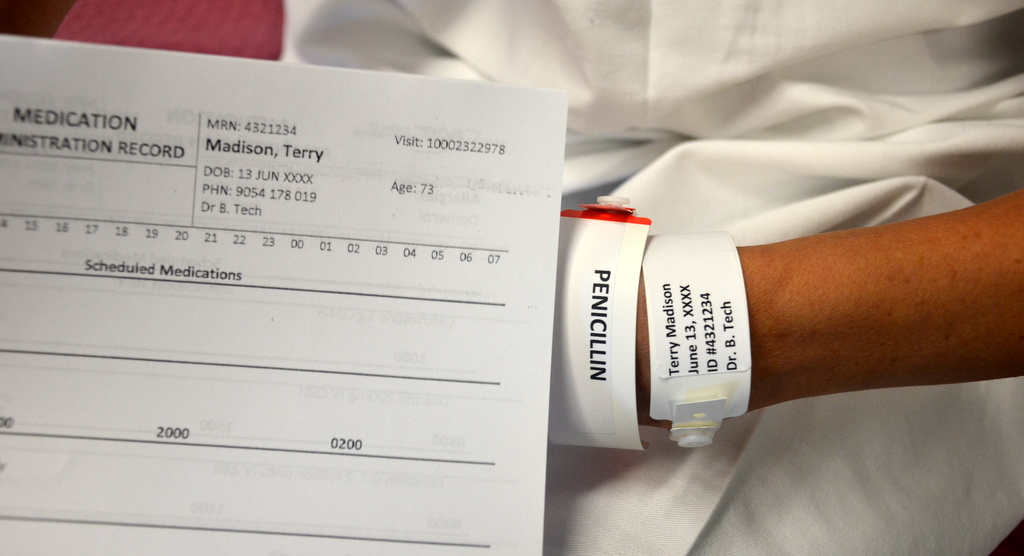
- Safeguards for medication administration exist in most hospitals. Make use of all safety strategies (such as smart IV pumps, no-interruption zones, two patient identifiers, and checklists) to administer medications safely.
- Quality and safety controls for safe medication administration must be considered along the entire process, not just at the point of administration.
- It is human nature to look for quick and easy ways to perform a task, but doing so may lead to errors. Avoid workarounds: Most hospitals have operational failures that lead to front line health care providers finding ways to manage deficiency in hospital operating systems. Rather than creating workarounds, engage in the additional steps to prevent re-occurrence of issues.
- Stay current with evidence-based research regarding potential system errors in health care. Commit to improving patient safety with medication administration.
- Report all errors, near misses, and adverse reactions to ensure knowledge is shared, and to prevent further errors from occurring.
Suggested Online Resources
- Agency for Healthcare Research and Quality (AHRQ). This website provides evidence-based research, guidelines, recommendations, and resources on improving patient safety.
- Canadian Patient Safety Institute (CPSI). This organization’s website provides guidelines, research, and recommendations for improving patient safety in Canada.
- Drug calculations. This medication calculation website reviews how to calculate the dosages for parenteral and non-parenteral medications, and IV fluids. It also includes metric conversions and IV drop rate calculations.
- Institute for Healthcare Improvement (IHI). This group’s website provides educational resources, webinars, publications, and improvement stories and tools to enhance patient safety.
- Institute for Safe Medication Practices (ISMP). This organization focuses on improving medication administration. The website lists high-alert medications, offers newsletters and webinars, and provides a system for reporting medication errors, guidelines, and policies on safe practices.
References
Ağac, E., & Günes, U. Y. (2011). Effect on pain of changing the needle prior to administering medication intramuscularly: A randomized controlled trial. Journal of Advanced Nursing, 67(3), 563-568. doi: 10.1111/j.1365-2648.2010.05513.x.
Agency for Healthcare Research and Quality. (2014). Checklists. Retrieved from http://psnet.ahrq.gov/primer.aspx?primerID=14.
Alberta Health Services. (2009). Direct IV medications. Specialized clinical competency program. Retrieved from http://extcontent.covenanthealth.ca/Policies/iii-45_Learning_Module.pdf.
American Nurses Association. (2002). Needlestick prevention guide. Retrieved from http://www.who.int/occupational_health/activities/2needguid.pdf.
Astle, B., & Duggleby, W. (2019). Canadian fundamentals of nursing (6th ed.). Milton, ON: Elsevier.
Becton, Dickinson UK. (2013). Hidden talents of BD Saf-T-Intima. Retrieved from https://www.bd.com/europe/safety/en/pdfs/Saf-T-Intima%20use%20Guide.pdf.
Berman, A., & Snyder S. J. (2016). Skills in clinical nursing (8th ed.). Hoboken, NJ: Pearson.
Black, L. (2013). Ditch the pinch: Bilateral exposure injuries during subcutaneous injections. American Journal of Infection Control, 41(9), 815-819. doi: 10.1016/j.ajic.2012.10.017.
British Columbia Institute of Technology (BCIT). (2015). Week 11 PowerPoint notes. In, NURS 3020: Clinical Techniques. Vancouver, BC: BCIT.
Brookside Associates. (2015a). Procedure for administering an intradermal injection. Retrieved from http://brooksidepress.org/intramuscular/lessons/lesson-2-administer-an-intramuscular-injection/2-07-procedure-for-administering-an-intradermal-injection/.
Brookside Associates. (2015b). Procedure for administering a subcutaneous injection. Retrieved from http://brooksidepress.org/intramuscular/lessons/lesson-2-administer-an-intramuscular-injection/2-05-procedure-for-administering-a-subcutaneous-injection/.
Butt, A. R. (2010). Medical error in Canada. Issues related to reporting medical error and methods to increase reporting. McMaster University Medical Journal, Clinical Review, 7(1), 15-18.
Canadian Agency for Drugs and Technologies in Health. (2014). Aspirating versus not aspirating prior to injection of medication: Comparative clinical evidence and guidelines. Retrieved from
https://www.cadth.ca/sites/default/files/pdf/htis/nov-2014/RB0669%20Aspiration%20Prior%20to%20Injection%20Final.pdf.
Canadian Diabetes Association. (2013). Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Clinical practice guidelines for the prevention and management of diabetes in Canada. Canadian Journal of Diabetes, 37(1), s1-s212.
Canadian Institute for Health Information. (2009). National system for incident reporting: An innovative approach to information management [CPSI Forum, April 29, 2009]. Retrieved from http://www.patientsafetyinstitute.ca/English/toolsResources/Presentations/Documents/2009/Canada%27s%20Forum%20-%20Presentation%20A4-b.pdf
Canadian Patient Safety Institute. (2012). Canadian analysis incident framework. Retrieved from http://www.patientsafetyinstitute.ca/english/toolsresources/incidentanalysis/documents/canadian%20incident%20analysis%20framework.pdf.
Centers for Disease Control (CDC). (2012). NOISH fast facts (home healthcare workers). How to prevent needlestick and sharps injuries. Retrieved from http://www.cdc.gov/niosh/docs/2012-123/pdfs/2012-123.pdf.
Centers for Disease Control (CDC). (2013). Infection control. Retrieved from http://www.cdc.gov/oralhealth/infectioncontrol/faq/protective_equipment.htm.
Centers for Disease Control (CDC). (2015). Injection safety. Retrieved from http://www.cdc.gov/injectionsafety/.
Children’s Hospitals and Clinics of Minnesota. (2018). Infiltration and extravasation care. Retrieved from https://www.childrensmn.org/educationmaterials/childrensmn/article/16565/infiltration-and-extravasation-care/.
College of Nurses of Ontario. (2015). Medication practice standard. Retrieved from http://www.cno.org/Global/docs/prac/41007_Medication.pdf.
Clayton, B. D., Stock, Y. N., & Cooper, S. E. (2010). Basic pharmacology for nurses. St. Louis, MO: Mosby Elsevier.
Cocoman, A., & Murray, J. (2008). Intramuscular injections: A review of best practice for mental health nurses. Journal of Psychiatry Mental Health Nursing, 15(5), 424-434. doi: 10.1111/j.1365-2850.2007.01236.
Davidson, K. M., & Rourke, L. (2014). Teaching best evidence: Deltoid intramuscular injection techniques. Retrieved from http://www.sciedu.ca/journal/index.php/jnep/article/view/1888/1291.
Debono, D. S., Greenfield, D., Travaglia, J. F., Long, J. C., Black, D., Johnson, J., & Braithwaite, J. (2013). Nurses’ workarounds in acute healthcare settings: A scoping review. BMC Health Services Research, 13(175). doi: 10.1186/1472-6963-13-175.
Ellis, J., & Parush, A. (2012). Preventing errors with high alert drugs: Testing a computerized double check. Retrieved from http://www.patientsafetyinstitute.ca/English/research/cpsiResearchCompetitions/2009/Documents/Ellis/Ellis%20Techinical%20Report%20English.pdf.
Greenway, K. (2014). Rituals in nursing: Intramuscular injection. Journal of Clinical Nursing, 23(23-24), 3583-3588. doi: 10.1111/jocn.12627.
Goossens, G. (2015). Flushing and locking of venous catheters: Available evidence and evidence deficit. Nursing Research and Practice, 2015(985686). https://dx.doi.org/10.1155%2F2015%2F985686.
Health Canada. (2012). Adverse reaction information. Retrieved from http://www.hc-sc.gc.ca/dhp-mps/medeff/advers-react-neg/index-eng.php.
Hunter, J. (2008). Intramuscular injection techniques. Nursing Standard, 22(24), 35-40.
Hutin, Y., Hauri, A., Chiarello, L., Caitlin, M., Stillwell, B., Ghebrehiwet, T., Garner, J., & Members of the Safe Injection Practices Development Group (2003). Best infection control practices for intradermal, subcutaneous, and intramuscular injections. Retrieved from http://www.who.int/bulletin/volumes/81/7/Hutin0703.pdf.
Institute for Healthcare Improvement. (2015). High-alert medication safety. Retrieved from http://www.ihi.org/topics/highalertmedicationsafety/pages/default.aspx.
Institute for Safe Medication Practices (ISMP). (2003). How fast is too fast for IV push medications? Journal of Radiology Nursing, 28(2), 66. https://doi.org/10.1016/j.jradnu.2007.05.002.
Institute for Safe Medication Practices (ISMP). (2013). Independent double checks: Undervalued and misused: Selective use of this strategy can play an important role in medication safety. Retrieved from https://www.ismp.org/resources/independent-double-checks-undervalued-and-misused-selective-use-strategy-can-play.
Institute for Safe Medication Practices (ISMP). (2014). ISMP list of high alert medications in acute care settings. Retrieved from https://www.ismp.org/tools/highalertmedications.pdf.
Institute for Safe Medication Practices Canada (ISMP Canada). (2014a). Ontario hospital critical incident related to medications or IV fluids analysis report: January to December 2013. Retrieved from http://www.ismp-canada.org/download/ocil/ON_Critical_Incidents_Analysis_Report_3JUL2014.pdf.
Institute for Safe Medication Practices Canada (ISMP Canada). (2014b). Opioid-related deaths associated with medication incidents. Findings of multi-incident analysis. Retrieved from http://www.ismp-canada.org/download/OpioidStewardship/Opioid-Related_Deaths_Associated_with_Medication_Incidents_Nov2014.pdf.
Ipp, M., Sam, J., & Parkin, P. C. (2006). Needle aspiration and intramuscular vaccination. Archives of Pediatrics and Adolescent Medicine, 160(4), 451-453. doi: 10.1001/archpedi.160.4.451-a.
Lynn, P. (2011). Photo atlas of medication administration (4th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Malkin, B. (2008). Are techniques used for intramuscular injection based on research evidence? Nursing Times, 104(50-51), 48–51.
Mitchell, J. R., & Whitney, F. W. (2001). The effect of injection speed on the perception of intramuscular injection pain. A clinical update. American Association of Occupational Health Nurses (AAOHN) Journal, 49(6), 286-292. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11760527.
National Institute for Occupational Safety and Health. (1999). ALERT: Preventing needlestick injuries in health care settings. Retrieved from http://www.cdc.gov/niosh/docs/2000-108/pdfs/2000-108.pdf.
National Institute of Health Clinical Center. (2015). NIH Clinical Center patient education material. Giving a subcutaneous injection. Retrieved from http://www.cc.nih.gov/ccc/patient_education/pepubs/subq.pdf.
National Patient Safety Agency. (2009). Safety in doses. Improving the use of medication in NHS. Retrieved from http://www.nrls.npsa.nhs.uk/resources/?entryid45=61625.
National Priority Partnership. (2010). Preventing medical errors: A $21 billion opportunity. Retrieved from http://psnet.ahrq.gov/resource.aspx?resourceID=20529.
Nisbet, A. C. (2006). Intramuscular gluteal injections in the increasingly obese population: Retrospective study. British Medical Journal, 332(7542), 637-638. http://dx.doi.org/10.1136/bmj.38706.742731.47.
Ogston-Tuck, S. (2014a). Intramuscular injection technique: An evidence-based approach. Nursing Standard, 29(4), 52-59. Retrieved from http://journals.rcni.com/doi/pdfplus/10.7748/ns.29.4.52.e9183.
Ogston-Tuck, S. (2014b). Subcutaneous injection technique: An evidence-based approach. Nursing Standard, 29(3), 53-58.
Öztürk, D., Baykara, Z., Karadag, A., & Eyikara, E. (2017). The effect of the application of manual pressure before the administration of intramuscular injections on students’ perceptions of postinjection pain: a semi-experimental study [PMID: 27535654]. Journal of Clinical Nursing, 26, 1632-1638. https://doi.org/10.1111/jocn.13530.
Parenteral. (2015). In Merriam-Webster on line dictionary. Retrieved from http://www.merriam-webster.com/medical/parenteral.
Perry, A., Potter, P., & Ostendorf, W. (2018). Clinical skills and nursing techniques (9th ed.). St. Louis, MO: Elsevier-Mosby.
Prakash, V., Koczmara, C., Savage, P., Trip, K., Stewart, J., McCurdie, T., … Trbovich, P. (2014). Mitigating errors caused by interruptions during medication verification and administration: Interventions in a simulated ambulatory chemotherapy setting. BMJ Quality and Safety, 23, 884-892. doi:10.1136/bmjqs-2013-002484
Pratt, J. R., Pellowe, C. M., Wilson, J. A., Loveday, H. P., Harper, P. J., Jones, S. R., … Wilcox, M. J. (2007). Epic2: National evidence based guidelines for preventing health care associated infections in NHS hospitals in England. Journal of Hospital Infection, 65(1), S1-64. https://doi.org/10.1016/S0195-6701(07)60002-4.
Provincial Infectious Disease Advisory Committee. (2014). Best practices for hand hygiene in all health care settings (4th ed.). Retrieved from http://www.publichealthontario.ca/en/eRepository/2010-12%20BP%20Hand%20Hygiene.pdf.
Rodgers, M. A., & King, L. (2000). Drawing up and administering intramuscular injections: A review of the literature. Journal of Advanced Nursing, 31(3), 574–582. doi: 10.1046/j.1365-2648.2000.01312.x.
Royal Children’s Hospital Melbourne (RCH). (2014). Subcutaneous catheter devices management of insuflon and BD safTIntima devices. Clinical Guidelines (Nursing). Retrieved from https://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/Subcutaneous_catheter_devices_management_of_insuflon_and_BD_safTIntima_devices/.
Saskatchewan Health Authority. (2018). Subcutaneous therapy – intermittent and continuous – adult & pediatric [catalogue no. 1074]. Policies & Procedures: Subcutaneous Therapy – Intermittent and Continuous. Retrieved from https://www.saskatoonhealthregion.ca/about/NursingManual/1074.pdf.
Sepah, Y., Samad, L., Altaf, A., Rajagopalan, N., & Khan, A. J. (2014). Aspiration in injections: Should we continue or abandon the practice? F1000Research, 3(157). 10.12688/f1000research.1113.1.
Siegel, J. D., Rhinehart, E., Jackson, M., Chiarello, L., & Healthcare Infection Control Practices Advisory Committee. (2007). Guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. Retrieved from http://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf.
Shah, K., Lo, C., Babich, M., Tsao, N., & Bansback, N. (2016). Bar code medication administration technology: A systematic review of impact on patient safety when used with computerized prescriber order entry and automated dispensing devices [PMID: 27826157]. Canadian Journal of Hospital Pharmacy, 69(5), 394-402. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5085324/.
Sisson, H. (2015). Aspirating during the intramuscular injection procedure: A systematic literature review. Journal of Clinical Nursing, 24(17-18), 2368-2375. https://doi.org/10.1111/jocn.12824.
Wilburn, S. Q. (2004). Needlestick and sharps injury prevention. The Online Journal of Issues in Nursing, 9(3). Retrieved from http://www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Volume92004/No3Sept04/InjuryPrevention.html.
Wilburn, S. Q., & Eijkemans, G. (2004). Preventing needlestick injuries among healthcare workers: A WHO-ICN collaboration. International Journal of Occupational and Environmental Health, 10(4), 451-456. https://doi.org/10.1179/oeh.2004.10.4.451.
Workers Compensation Act: Occupational health and safety regulation. (2015). BC Reg. 296/297. Retrieved from the BC Laws website: . http://www.bclaws.ca/Recon/document/ID/freeside/296_97_04.
Workman, B. (1999). Safe injection techniques. Nursing Standard, 13(39), 47-53. https://doi.org/10.7748/ns1999.06.13.39.47.c2623.
World Health Organization (WHO). (2012). Course: Knowledge is the enemy of unsafe care. Retrieved from http://who.int/patientsafety/education/curriculum/course7_handout.pdf.












































































































































































































































































































































































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.JPG){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.png){kind=link}
{kind=link}
{kind=link}
.png){kind=link}
{kind=link}
.jpg){kind=link}
![Nicoderm [patch]](https://fr.m.wikipedia.org/wiki/Fichier:Nicoderm.JPG){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Omläggning av PICC [Conversion of PICC]](https://commons.wikimedia.org/wiki/File:PICC_oml%C3%A4ggning.jpg){kind=link}
.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.png){kind=link}
{kind=link}